The New Default. Your hub for building smart, fast, and sustainable AI software

Table of Contents
There is no single best large language model for HealthTech. The decision that matters is which combination of models fits your clinical use case, your compliance obligations, and your deployment environment. Most production healthcare systems end up using more than one.
That answer frustrates people who want a leaderboard. But in healthcare, the leaderboard is the least interesting part of the problem.
A model that tops MedQA can still be the wrong choice if it forces protected health information (PHI) through an API you don't control, or if you can't explain its reasoning to a regulator. The decision space really has three axes: reasoning power, clinical accuracy, and data control. Optimizing one usually costs you another.
The most expensive mistakes in this space are the ones you discover in production. This guide will help you avoid them.
Executive summary
There is no single best LLM for HealthTech, and treating model choice as the first decision is how teams end up rebuilding at go-live.
The market splits into three categories (frontier general models, medically tuned models, and open-weight models you can self-host), and most real products combine them by function rather than picking one.
The binding constraint is rarely raw capability; it is your compliance boundary, meaning whether real patient data touches the model and under which regime. Benchmarks like MedQA tell you a model can reason clinically, but not that it will perform on your tasks, your patients, or your language.
Get the compliance architecture and human oversight right first, and the model becomes a swappable component rather than a bet.
Is It Difficult to Choose an LLM for HealthTech Products?
Yes, choosing an LLM is more difficult than picking one for less-regulated, less critical products.
If you're building a marketing tool and the model writes something clumsy, you edit it. The cost of failure is low. In healthcare, the cost of a wrong answer can be critical, and that changes the entire calculus of model selection.
Two things make HealthTech structurally different.
First, the PHI problem. The moment a model receives real patient data, your compliance obligations change completely. A comprehensive review of LLMs in healthcare published in Intelligent Medicine is blunt about this: patient privacy, data security, bias mitigation, and transparency are preconditions for responsible deployment. Most consumer SaaS API deployments do not clear that bar by default.
Second, the stakes are already real, whether you're ready or not. A Nature study analyzing more than 500,000 de-identified health conversations with Microsoft Copilot in January 2026 found that nearly one in five conversations involved personal symptom assessment or discussion of a specific condition. One in seven of those personal queries was about someone other than the user, a sign people are already using general chatbots as caregiving tools. Personal health queries spiked in the evening and at night, exactly when traditional care is least available. People are bringing health questions to general-purpose AI right now. The question is whether the products you build to meet them are designed for it.
Teams prototype fast with a frontier API, validate the user experience, and get excited. Then at production they discover that the compliant, on-premise version they actually need was never feasibility-tested. The model choice set the data-flow design, which set the compliance posture, which determined whether they could ship at all. That chain runs in one direction, and it's cheaper to reason about it up front.
Three Categories of LLMs to Use In Digital Products
Almost every model you'll consider falls into one of three buckets. Understanding what each is good and bad at is most of the battle.
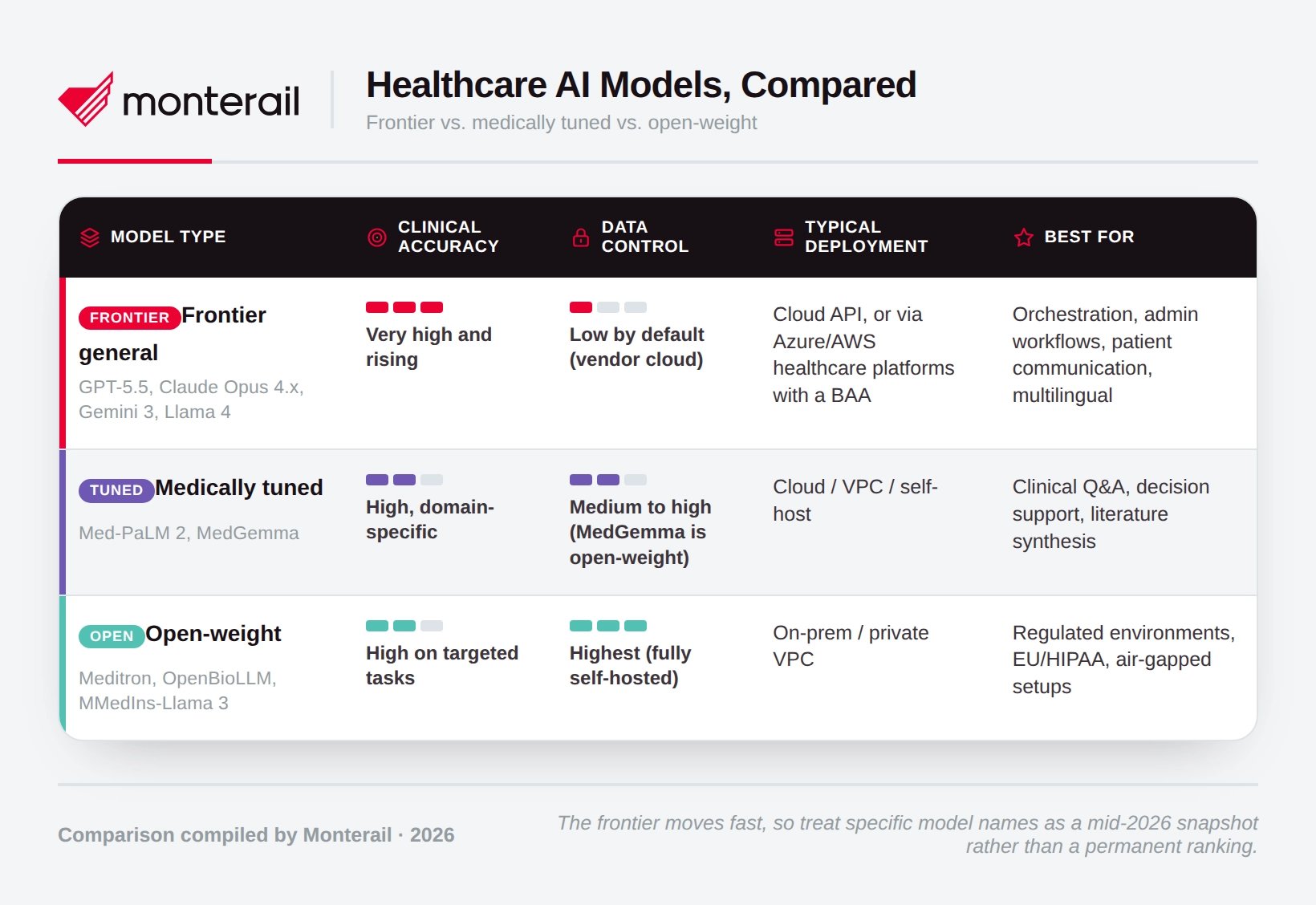
1. Frontier general models
These are the models most people already know: the current frontier includes GPT-5.5, Claude Opus 4.x, Gemini 3, and the open-weight Llama 4. They aren't trained specifically for medicine, but they are extraordinarily capable at reasoning, following instructions, using tools, and working across languages.
For years, the accepted wisdom was that these models trailed specialized medical models on clinical benchmarks. That's no longer safe to assume. A 2026 Nature Medicine study found that general-purpose frontier LLMs outperformed specialized clinical AI tools across its evaluations. General models like GPT-5 now report MedQA scores around 95%, above the roughly 91% that Google's research model Med-Gemini reported (Med-Gemini details here). The specialized advantage has eroded as the frontier has advanced.
These models excel at orchestration and workflow reasoning, administrative and non-clinical content, multilingual patient communication, and acting as the brain that coordinates retrieval and tools.
But be careful! By default, using them means sending your data to someone else's cloud, which is a compliance decision and not just a technical one (more on that below).
2. Medically tuned models
These are models trained or fine-tuned on clinical guidelines, biomedical literature, and medical exam data. Google's Med-PaLM 2 reached expert-level performance on USMLE-style questions, and its successor line pushed further. For teams that want to actually build on a Google medical model, the practical option today is MedGemma, an open collection released on Gemma 3 and updated to MedGemma 1.5 in January 2026. Its 27B text variant scores around 87.7% on MedQA, and the multimodal variants handle medical imaging.
Just remember that medical benchmarks are imperfect. When Google's clinicians inspected MedQA, they found that 7.4% of the questions were unfit for evaluation, because they were missing key information or supported multiple plausible answers. A high score on a flawed test is not the same as clinical reliability.
These models excel at clinical question-answering, decision support, pharmacology, and literature synthesis where domain knowledge genuinely matters.
However, you might encounter issues with access constraints (some of the strongest medical models are research artifacts or partner-only) and the temp tation to trust a benchmark number as a clinical guarantee.
3. Open-weight models you can self-host
Open medical models let you run everything inside your own infrastructure, so no patient data ever leaves your control.
The strongest examples are built on Meta's Llama family. Meditron, from EPFL, Yale, and the ICRC, was designed explicitly for clinical decision support in low-resource settings. Its Llama-3.1-based suite reports outperforming other open and several closed models on MedQA, MedMCQA, and PubMedQA, with weights and data openly available. OpenBioLLM-70B and instruction-tuned models like MMedIns-Llama 3 have likewise reported beating larger proprietary models on specific biomedical tasks.
These models are great for HIPAA/GDPR-constrained deployments, EU data residency, air-gapped hospital environments, and any workload where "no PHI leaves our walls" is non-negotiable.
Just watch out for infrastructure cost. A 70B-parameter model is real hardware, and you own the MLOps burden that a SaaS API would otherwise absorb.
Comparison of HealthTech AI Models
Which LLM for Different HealthTech Tasks?
The three categories become actionable once you map them to what you're actually building.
Rapid proof-of-concept on non-PHI data. Start with a frontier API plus retrieval (RAG) over your own medical content, such as guidelines, care pathways, and formularies. It's fast, cheap, and good enough to validate the workflow and UX. The one rule: no real patient data until the compliance work is done.
Clinician-facing decision support. This needs a medically tuned or strong frontier model, sitting behind retrieval from current clinical guidelines and local protocols, with a human in the loop. The healthcare review is emphatic that human oversight is not optional, because hallucinations here have direct clinical consequences. Design the oversight before you pick the model.
Patient-facing applications. A frontier model gives you conversational quality; a medical model or RAG layer supplies the clinical substance. What matters most is scope and safety: no diagnosis, clear escalation paths to human care, and readability tuned to real patients. The same review notes that LLM outputs often exceed patients' comprehension levels, and accuracy is wasted if the patient can't understand the answer.
Clinical NLP and EHR workflows. For ICD coding, named-entity recognition, de-identification, and note summarization, smaller task-specific models frequently beat large general ones, and dedicated clinical NLP stacks packaged for on-prem, HIPAA/GDPR-compliant use are often the pragmatic choice. This is structured extraction rather than open-ended chat, so right-size the model to the task.
Pharma and biotech R&D. Large open biomedical models shine here for literature Q&A, knowledge-graph work, and research synthesis. As a broad review of LLMs in biomedicine documents, the applications now reach deep into genomics, transcriptomics, and proteomics. Expect to provision serious GPU capacity for 70B-class models run in-house.
What You Need To Fix Before Integrating LLMs
Model selection is the output of these decisions, not the input. Resolve them first.
Define the compliance boundary. The single most important question is whether PHI will reach the model. If yes, you need either self-hosting or a signed Business Associate Agreement (BAA) with your provider. "HIPAA-eligible" is not the same as "compliant," either. Both major vendors now offer healthcare paths: OpenAI launched OpenAI for Healthcare in January 2026, with a BAA available only to sales-managed ChatGPT Enterprise and Edu accounts and explicitly not HIPAA-compliant out of the box; Anthropic offers HIPAA-ready Enterprise plans and BAAs for qualifying API customers. Read the fine print: the covered products and the effective dates matter.
Confirm data residency. GDPR and national health laws often require EU-resident infrastructure. A US-hosted model may be a non-starter regardless of how good it is, and cloud contracts need real legal review rather than a checkbox.
Understand the EU AI Act early. For teams serving Europe, AI systems that are, or are embedded in, devices regulated under the MDR or IVDR are automatically classified as "high-risk" under the AI Act. That brings obligations for risk management, transparency, cybersecurity, and human oversight on top of existing device rules. Timelines have shifted under the proposed Digital Omnibus package, with high-risk obligations for embedded medical AI now extending toward 2027–2028, but the direction is clear. Designing for it now is far cheaper than retrofitting.
Build for explainability. A 2025 Nature analysis argues that in regulated healthcare, interpretability alone is no longer enough: transparency, fairness, and trust are becoming regulatory requirements, not nice-to-haves. Because LLMs are generative and stochastic, the same input can produce different outputs, so plan for source attribution, logging, and traceable reasoning from day one.
Cost the infrastructure honestly. Self-hosting a 70B model is a hardware commitment. If an open model is your primary plan, price the GPUs, the inference scaling, and the MLOps before you commit, not after.
Benchmark on your own data. Public scores are a proxy. Run your own evaluation on your specialties, your languages, and your task types. Medical benchmarks are overwhelmingly English and exam-shaped; your product is neither.
What To Do When Starting a New HealthTech Build?
When a HealthTech team comes to us with a blank page, the sequence usually looks like this. Prototype quickly with a frontier model plus retrieval over the client's own clinical content, enough to validate that the workflow actually fits how clinicians or patients behave. In parallel, not afterwards, benchmark one or two open medical models on the client's real tasks and languages, and pressure-test whether an on-prem, EU-resident deployment is feasible for go-live.
From the very first sprint, design the parts that are hard to change later: human oversight, audit logging, explanation, and a tightly scoped clinical remit.
The pattern that keeps teams out of trouble is treating the model as swappable and the architecture as durable. Models improve every few months; a well-designed compliance and governance layer lets you adopt the next one without rebuilding.
At Monterail, we help HealthTech and MedTech teams turn this framework into a working product: choosing the right model stack, designing a compliant, EU-ready architecture, and building the retrieval, oversight, and governance layers that make clinical AI trustworthy. If you're weighing these decisions for a new build, we're happy to talk through your specific use case and constraints.
Key takeaways
There is no single best HealthTech LLM. Production systems combine model types by function: general models for reasoning and orchestration, medical models for clinical depth, and open-weight models for data control.
Compliance is the binding constraint. Define whether PHI touches the model, and under which regime (HIPAA, GDPR, EU AI Act), before you shortlist anything.
Benchmarks inform; they don't decide. Evaluate on your own tasks, data, and languages, and remember that even flagship benchmarks like MedQA contain flawed questions.
The general-vs-specialized gap has narrowed. Frontier general models now rival or beat specialized clinical tools on many benchmarks, so re-examine assumptions from even a year ago.
Human oversight is architecture, not a feature. For any clinical use case, define who reviews, who overrides, and how errors are logged before choosing a model. No accuracy score removes that requirement.
HealthTech LLM FAQ
)
Piotr Zając
HealthTech Director
Piotr, Monterail’s Director of HealthTech brings over 15 years of entrepreneurial leadership and strategic innovation to the MedTech and HealthTech sectors. Piotr has demonstrated exceptional ability to build and scale healthcare solutions. Former President of EO Poland, part of the world's largest entrepreneur network. Combining his entrepreneurial background with Management 3.0 principles, Piotr specializes in helping organizations drive sustainable innovation in the rapidly evolving HealthTech landscape.